
Glaucoma
What is Glaucoma?
Glaucoma is the name given to a group of eye diseases that damage the Optic Nerve, most commonly resulting in the loss of peripheral vision. The Optic Nerve is responsible for transmitting visual information from the retina to the brain. Initially, the damage and effect is silent and painless. It has been termed the ‘thief of sight,’ as vision can be slowly ‘stolen’ over time. Symptoms with further loss can cause a darkening of the outer or peripheral vision, creating ‘tunnel vision.’ As the damage to the Optic Nerve increases the patients vision decreases and may lead to blindness.
Due to its initially asymptomatic nature, regular eye examinations are recommended every few years for everyone over the age of 40, and more frequently for those with a family history.
Glaucoma is the leading cause of irreversible blindness world wide and with currently over 300,000 Australians already diagnosed with glaucoma there will soon to be an increase in patients due to the population age increasing. While it is more common in patients over 50 it can occur at any age.
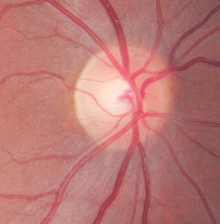
Example of a cupped disc

Example of a normal disc
Types of Glaucoma
- Primary Open Angle Glaucoma – this is the most commonly diagnosed form of Glaucoma relating to aging changes in the eyes. It is painless and the early signs may be a reduction of peripheral vision. It is caused by a blockage in the draining process of the fluid in the eye, called the aqueous humour. As the fluid struggles to freely move through the drainage system, called the trabecular meshwork, and into the blood steam it results in an increase in pressure inside the eye. Timely treatment is necessary because once damage has occurred to the optic nerve it is not possible to recover what has been lost, however, it is possible to slow down the progression. Hence early detection is vital.
- Low Tension or Normal Tension Glaucoma – is treated the same as primary Open Angle Glaucoma. Similar damage to the optic nerve can occur even when the pressure within the eye is normal.
- Congenital Glaucoma – is a rare form of Glaucoma caused by an abnormality in the drainage system of the eye. It can exist from birth but in some cases may develop later. A child may be observed from being sensitive to light and have enlarged and cloudy eyes. Surgery is the most common form of treatment with this type of Glaucoma.
- Secondary Glaucoma – develops as a result of non-age related insults to the eye. There can be many different causes ranging from trauma, inflammation, medications, retinal vascular disorders (such as central retinal vein occlusion) and diabetes.
- Acute Closed Angle Glaucoma – this is a very painful form of Glaucoma that occurs when there is a blockage at the pupil. The normal, healthy fluid circulation throughout the eye then builds up abruptly behind the iris pushing it forward to obstruct the drainage system resulting in high pressure. Sudden loss of vision and extreme pain in the eye will occur as well as in many cases a feeling of nausea and vomiting. This is an ocular emergency and immediate assessment is required. People of Asian origin and extreme long sightedness (hyperopia) are at particular risk.
Symptoms & Diagnosis
As mentioned above, the majority of Glaucoma’s develop slowly without pain. The major exception is Acute Angle-Closure Glaucoma which presents with an acute red eye, blurred vision and may include severe pain, nausea and vomiting. Otherwise, visual symptoms due to Glaucoma are usually only experienced when the condition is relatively advanced.
Regular eye examinations are recommended to detect if there is any sign of damage or deterioration to the optic nerve fibres. Once damage has been done to the optic nerve it is irreversible and your Ophthalmologist can only control and ideally halt or slow the progression of the disease with either a series of ongoing treatments or surgery.
People at a higher risk of Glaucoma developing include those with:
- Family history of Glaucoma
- High intraocular pressure
- High blood pressure
- Migraines
- Diabetes
- Previous trauma to the eye
- Peripheral vascular disease
- High refractive error (long or short sightedness)
- Thin corneas (may indicate a falsely low intraocular pressure)
There is no one single test that will diagnose Glaucoma, and other conditions can mimic Glaucoma. The ophthalmic technicians will conduct a series of tests including:
- Field test; checks the peripheral vision
- Optical Coherence Tomography; images of the retina and the optic nerve
- Pachymetry; measures the corneal thickness
- Disc photos; taking images of the optic disc at the back of the eye
Management
Although there is no cure for Glaucoma it is usually controlled with a range of treatments. Primarily the focus of treatment is to prevent further damage occurring to the optic nerve and avoiding permanent blindness. Fortunately there is a range of treatment options available to control Glaucoma of which the most appropriate option will be determined by your Ophthalmologist best suited to your individual needs. Patients suffering from Glaucoma will need to be reviewed on a regular basis to enable the Ophthalmologist to monitor their eyes and make sure that their Glaucoma is being managed correctly.
Treatment options at the Launceston Eye Institute include the following:
- Eye Drops – are the most common form of treatment for Glaucoma, however to be effective the eye drops are a life long commitment and are to be used regularly. There are a variety of eye drops available that are designed to lower the intraocular pressure and reduce the progression of the Glaucoma. Depending on the type of Glaucoma, and the stage of its progression, your Ophthalmologist will determine the most suitable form of eye drops.
- Selective Laser Trabeculoplasty (SLT) – the SLT is generally performed when the intraocular pressure has not reduced to a normal level with the regular use of eye drops. It is a minor procedure performed under local anaesthetic in the rooms at the Launceston Eye Institute and does not require admission to hospital. The laser trabeculoplasty is used to assist the drainage of the aqueous humour by unblocking the trabecular meshwork to assist the flow from the eye. Commonly after the laser trabeculoplasty eye drops are still required to reduce the intraocular pressure and slow the progression of the Glaucoma.
- Surgery – for most forms of Glaucoma surgery is performed after the eye drops and the laser have been unsuccessful in controlling the intraocular pressure except in the case of acute closed-angle Glaucoma and Congenital Glaucoma where surgery may be required immediately. In most cases no further medication is required after surgery. The surgery aims to create a new channel for the fluid to drain reducing the intraocular pressure and bypassing the blockage of the trabecular meshwork.
Important Notes
- Glaucoma is a disease of the optic nerve
- It is more common with age, but can affect children, adults and the elderley and can take many forms
- Commonly, there may be no noticeable alteration of vision, however, once damage or vision loss occurs, it cannot be reversed
- Tests of intraocular pressure, peripheral visual field and scans of the structure of the eye are necessary for diagnosis and at regular intervals to ensure there has been no progression (deterioration)
- Treatment is aimed at lowering the intraocular pressure, but this is typically individualised to each patient
- Treatment options include drops, laser or surgery
- Treatment is typically life long, once diagnosis is confirmed